Last updated on May 20, 2026
CMS Medicare Authorization to Disclose Personal Health free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is CMS Medicare Authorization to Disclose Personal Health
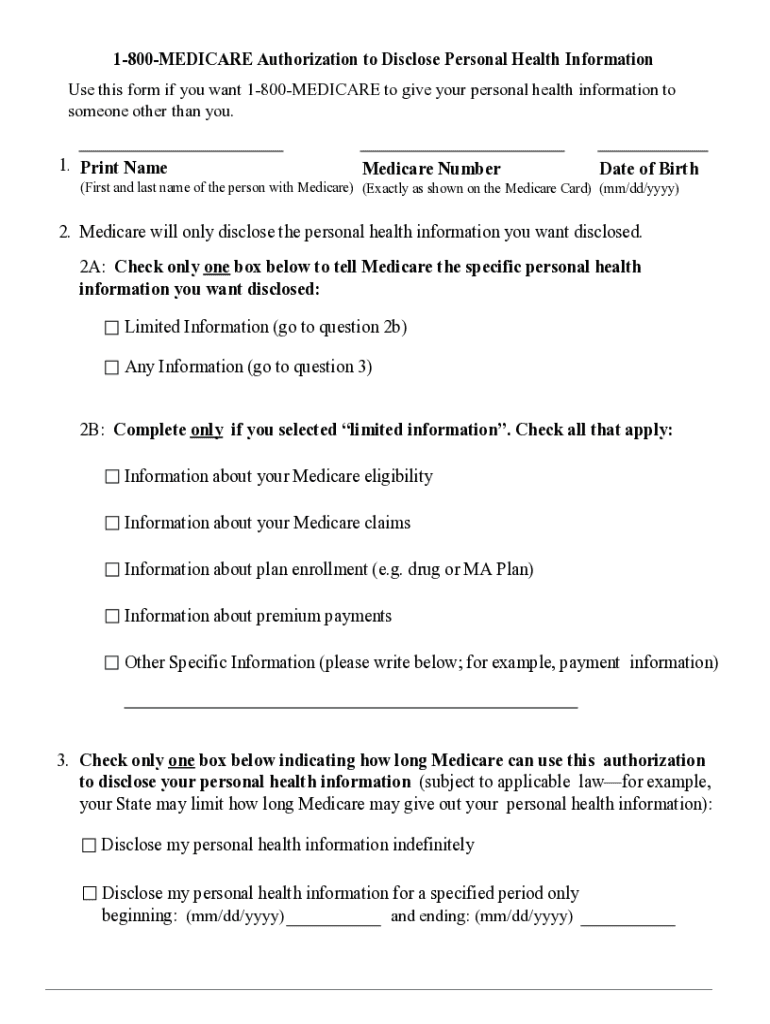
The Medicare Authorization to Disclose Personal Health Information is a healthcare form used by Medicare beneficiaries to grant permission for the disclosure of their personal health information to specified individuals or organizations.
pdfFiller scores top ratings on review platforms
This is an excellent tool that helps me in my small business.
I found the system complicated for someone not very experienced with computers. I still do not know how to find, on your system, the forms that I have completed. Where are they? How do I save them to my computer? I will keep working to find the answers.
Who needs CMS Medicare Authorization to Disclose Personal Health?
Explore how professionals across industries use pdfFiller.

CMS Medicare Authorization to Disclose Personal Health is needed by:
-
Medicare beneficiaries wanting to share health information
-
Personal representatives handling health matters
-
Healthcare providers requiring access to patient information
-
Family members assisting with medical decisions
-
Legal guardians involved in healthcare decisions
Comprehensive Guide to CMS Medicare Authorization to Disclose Personal Health
Understanding the Medicare Authorization to Disclose Personal Health Information
The Medicare Authorization to Disclose Personal Health Information form is a critical document for beneficiaries wishing to share their personal health details. This form allows Medicare recipients to grant permission for selected individuals or organizations to access their health information. It is essential for ensuring proper communication between beneficiaries and healthcare providers, as it establishes a legal framework for information sharing. By completing this form, beneficiaries can stipulate exactly what personal health information may be disclosed, highlighting its significant role within the Medicare system.
Granting permission for disclosure is vital. Without this authorization, healthcare providers may be restricted from accessing necessary information, potentially affecting the quality of care received. This form is especially crucial for Medicare beneficiaries to facilitate communication concerning their health management.
Who Needs to Complete the Medicare Authorization to Disclose Personal Health Information?
Individuals who qualify as a “Person with Medicare” or their “Personal Representative” should consider completing this authorization form. A “Person with Medicare” refers to individuals who are enrolled in the Medicare program, while a “Personal Representative” may include legal guardians or individuals designated to make health decisions on the beneficiary's behalf.
The form is necessary in various scenarios, including when beneficiaries wish to share their health information with healthcare providers, family members, or legal representatives. It addresses the legal implications involved, making it clear that both parties are responsible for the information disclosed through the form.
Key Features of the Medicare Authorization to Disclose Personal Health Information Form
This authorization form includes essential fields that must be completed accurately. Required fields include the beneficiary's name, Medicare number, and date of birth to ensure proper identification. Moreover, it outlines specific details on what health information can be shared, which is crucial for maintaining clarity in communication.
For residents of New York, the form also incorporates state-specific instructions to adhere to privacy laws unique to this region. These features ensure compliance and protect beneficiaries' health information effectively.
How to Fill Out the Medicare Authorization to Disclose Personal Health Information Online
Filling out the Medicare Authorization form online is straightforward with the following steps to guide you:
-
Access the form online and ensure you have your Medicare number, name, and date of birth at hand.
-
Complete each required field carefully, inputting the necessary personal information.
-
Follow the specific instructions for the type of information you wish to disclose.
-
Review your entries for accuracy to minimize errors before submission.
-
Submit the completed form electronically or print and mail it as needed.
Before beginning, gather the necessary information to streamline the process. Common errors include incorrectly entering the Medicare number or failing to sign the form, so careful attention is crucial.
Submission Methods for the Medicare Authorization to Disclose Personal Health Information
Once the form is completed, you have several methods to submit it for processing. The available submission methods include:
-
Mailing the form directly to Medicare.
-
Submitting the completed form online through authorized platforms.
Be aware of any applicable fees and the estimated processing time, which can vary. After submission, confirming receipt of the form is recommended to ensure it is being processed correctly, along with understanding the next steps following submission.
Privacy and Security Considerations When Using the Medicare Authorization Form
Handling sensitive information necessitates strict privacy and security measures. The Medicare Authorization form uses advanced data protection techniques to secure submissions. These measures align with HIPAA compliance and emphasize the need for responsible handling of health information.
Beneficiaries must understand their privacy rights when sharing personal health information. Awareness of how data is managed and protected is crucial for safeguarding sensitive health data throughout the authorization process.
What Happens After Submission of the Medicare Authorization to Disclose Personal Health Information
After sending the completed authorization form, beneficiaries should anticipate certain steps:
-
Processing of the form typically takes a few weeks, during which Medicare will confirm acceptance.
-
Beneficiaries can check the status of their submitted authorization, ensuring transparency in the process.
-
If corrections or amendments are necessary, beneficiaries should understand the procedures to adjust their submissions.
Utilizing pdfFiller for Your Medicare Authorization Form Needs
pdfFiller significantly simplifies the process of filling and submitting the Medicare Authorization to Disclose Personal Health Information form. The platform offers features to create a fillable form, enhancing user experience and efficiency.
With robust security measures in place—such as encryption and compliance with privacy regulations—users can trust that their information remains safeguarded. Consider using pdfFiller's tools to streamline your form filling and submission process effectively.
How to fill out the CMS Medicare Authorization to Disclose Personal Health
-
1.Access pdfFiller and search for 'Medicare Authorization to Disclose Personal Health Information' in the form finder.
-
2.Open the form by clicking on the title once you locate it in the search results.
-
3.Ensure you have your Medicare number, name, and date of birth ready before starting to fill out the form.
-
4.Begin by entering your personal information in the designated fields, paying close attention to accuracy.
-
5.Check the boxes that are applicable for the health information you wish to disclose and the individuals or organizations authorized to receive it.
-
6.Scroll through the form carefully, ensuring that all required fields are filled out completely.
-
7.Review the complete form for any potential errors, and verify all the details are correct and up to date.
-
8.Once satisfied with the information provided, save your progress to prevent data loss.
-
9.You may download the completed form, or directly submit it to Medicare via the provided submission option on pdfFiller.

Who is eligible to use the Medicare authorization form?
The Medicare Authorization to Disclose Personal Health Information can be used by any Medicare beneficiary who wishes to share their health information with designated individuals or organizations.
Are there any deadlines for submitting this form?
It is advisable to submit the Medicare authorization form as soon as possible to avoid delays in accessing necessary health services. Always check with your healthcare provider about specific deadlines.
How can I submit the completed form?
You can submit the completed Medicare authorization form through pdfFiller by using their integrated submission method, or by downloading and sending it directly to Medicare via mail.
What supporting documents are required with this form?
Generally, no additional supporting documents are required with the Medicare Authorization to Disclose Personal Health Information. However, you may need to provide identification if requested.
What are common mistakes to avoid when completing the form?
Common mistakes include missing signatures, incorrect Medicare number entries, and failing to specify which information to disclose. Ensure all fields are carefully filled out.
How long does it take for the form to be processed?
Processing times for the Medicare authorization form may vary. Typically, it can take a few weeks for Medicare to process the request and update their records.
What if I need to change my permissions after submitting the form?
If you need to change your permissions after submitting the Medicare authorization form, you will have to complete a new authorization form and submit it according to the same procedures.
Related Content
Related Forms


Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.